What is an Osteopathic Sieve?
"Freddie, when I come in with a sore back, what are you actually doing in those first few minutes? You ask a lot of questions before you even touch anything."
Freddie: "Those questions are probably the most important part of the whole session. Before we treat anything, we need to rule out the things that shouldn't be treated — at least not by us, and not right now."
What is the osteopathic sieve?
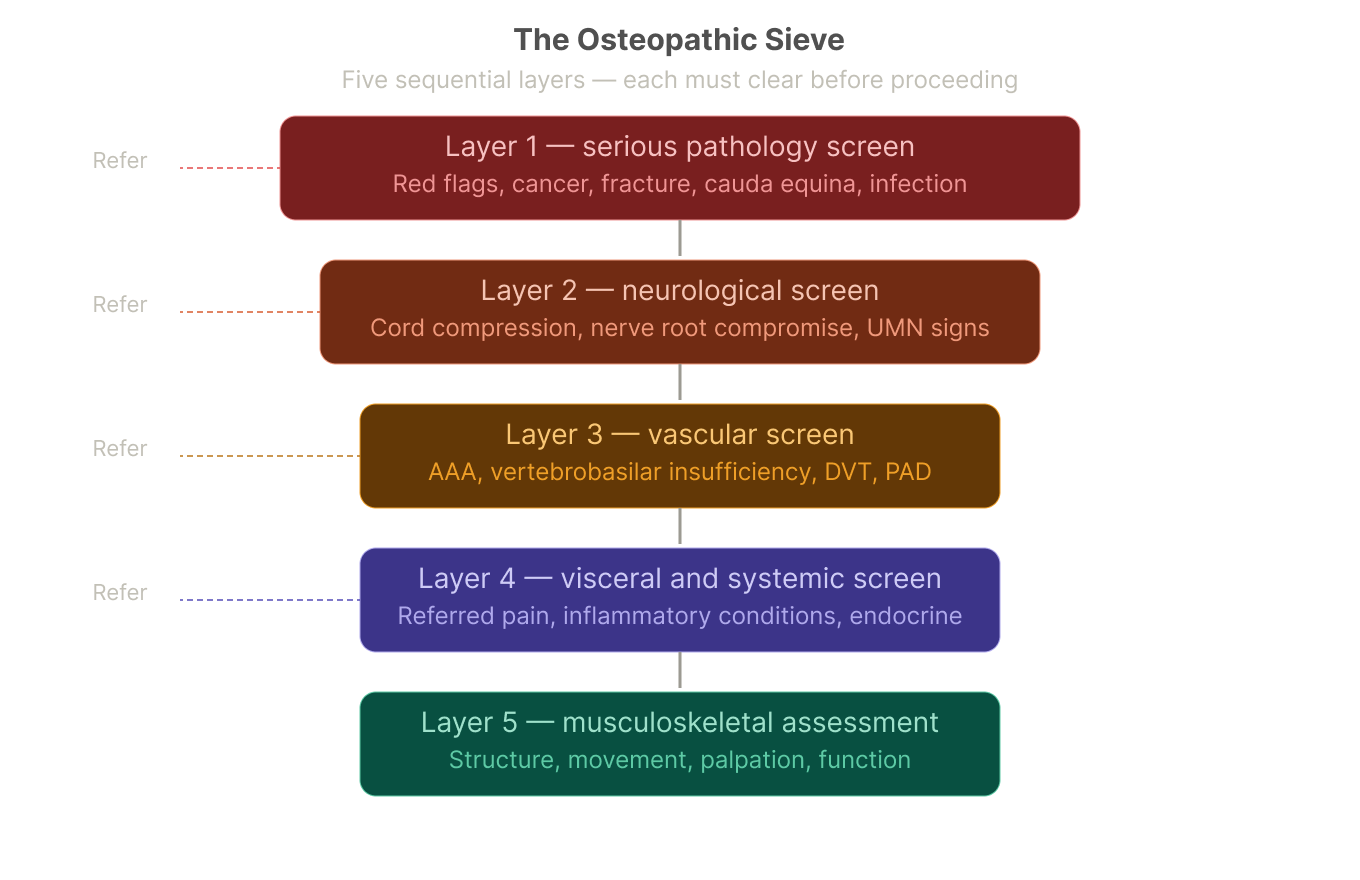
The osteopathic sieve is a systematic clinical screening framework used at the start of every assessment. It is a sequential filter — five layers, each progressively more specific — that helps the clinician determine whether the complaint in front of them is appropriate for osteopathic management, needs onward referral, or requires urgent medical attention.
The word "sieve" is deliberate. Just as a sieve separates coarse material from fine, the assessment separates conditions that require a different clinical pathway from those that are appropriate to treat. Each layer must clear before we proceed to the next.
This is not bureaucracy. It is the clinical and ethical foundation of safe practice.
The sieve sits within the broader osteopathic examination structure — history, physical examination, special orthopaedic and neurological tests, and osteopathic palpation. But the sieve layers come first, because missing them has the most serious consequences.
The five layers, and why each one matters
The diagram above shows the full structure. Here is what each layer is doing clinically.
-
This is the most critical layer. It screens for conditions where the presenting pain or symptom has a sinister, non-mechanical cause — one that requires urgent referral rather than manual treatment.
The clinical red flags we screen for include:
Unexplained weight loss, night sweats, fever — possible malignancy or infection
Pain that is constant, progressive, and not relieved by rest or position change
History of cancer — spinal or bony metastases can mimic mechanical back pain precisely
Age of first onset over 50 with no previous history — raises suspicion for malignancy or serious systemic disease
Bilateral neurological symptoms, bowel or bladder dysfunction — cauda equina syndrome, a surgical emergency
Recent significant trauma, especially in an older patient — possible fracture
Unremitting pain at rest or night pain that wakes from sleep — potential serious spinal pathology
The clinical literature underpinning this layer is extensive. Deyo and Diehl (1988, Annals of Internal Medicine) established the original red flag criteria for low back pain, later refined by multiple guidelines including the NICE low back pain guideline (2016) and the Australian Commission on Safety and Quality in Health Care (2018).
If red flags are present, we refer immediately and do not treat.
-
Once serious pathology is cleared, we screen the neurological system. This has two components.
Upper motor neurone (UMN) signs: symptoms suggesting cord compression or central nervous system involvement. These include hyperreflexia, clonus, pathological reflexes (Babinski, Hoffmann), spasticity, and bilateral or multisegmental symptoms. UMN signs warrant urgent referral — they represent a level of neural compromise that is outside the scope of manual therapy.
Lower motor neurone (LMN) signs and nerve root compromise: dermatomal pain patterns, myotomal weakness, reduced reflexes, and positive neurodynamic tests (straight leg raise, slump, upper limb tension tests). These require careful assessment. Nerve root compromise may well be appropriate for osteopathic management — but only once the nature and severity have been established clearly.
The neurological screen also informs the physical examination: which dermatomes and myotomes to test, which special tests are indicated, and how much load can be applied in treatment.
-
The vascular screen is perhaps the least visible but clinically important layer. Three conditions are particularly relevant to the musculoskeletal clinician.
Vertebrobasilar insufficiency (VBI): compromise of blood flow in the vertebral or basilar arteries, which supply the posterior brain. Relevant primarily to cervical spine assessment and treatment. The pre-manipulation screen for VBI — testing vertebral artery patency through sustained end-range rotation and extension — is standard practice before any cervical manipulation and is embedded in our assessment protocol. The International Federation of Orthopaedic Manipulative Physical Therapists (IFOMPT) published updated clinical guidelines for cervical artery dysfunction in 2020, which we follow.
Abdominal aortic aneurysm (AAA): a significant aneurysm can present as low back pain, sometimes with a pulsatile abdominal mass. Missed AAA with subsequent rupture is a medical catastrophe. Risk factors include age over 65, male sex, smoking history, and known vascular disease. The sieve prompts us to ask about these risk factors and, where indicated, palpate the abdominal aorta before any treatment.
Deep vein thrombosis (DVT) and peripheral arterial disease (PAD): relevant particularly to lower limb complaints. A calf that is swollen, warm, and tender in a patient with DVT risk factors (recent long-haul travel, surgery, immobility, oral contraceptive use) is a referral, not a massage.
-
This layer addresses referred pain and systemic conditions that present with musculoskeletal symptoms. It is clinically important because visceral pathology can mimic — sometimes perfectly — mechanical musculoskeletal pain.
Key examples:
Cardiac referred pain presenting as left arm, jaw, or inter-scapular pain — cardiac ischaemia must always be considered in thoracic or left shoulder complaints with appropriate risk factors
Renal colic presenting as acute lower back or flank pain with radiating groin pain — the presentation is often indistinguishable from L1 nerve root compromise without urine analysis
Pulmonary pathology presenting as thoracic or cervical pain — lung cancer, pleural effusion, and pulmonary embolism can all produce thoracic or shoulder pain
Gynaecological and pelvic pathology referring to the lower back, hip, or sacrum — endometriosis, ovarian cysts, and pelvic inflammatory disease are common causes of persistent low back or pelvic pain in women that is misattributed to a musculoskeletal source
Inflammatory arthropathies (ankylosing spondylitis, rheumatoid arthritis) presenting as spinal stiffness — morning stiffness lasting more than one hour, peripheral joint involvement, and a family history of inflammatory joint disease all suggest a rheumatological referral before manual treatment
The clinical red flags associated with this layer — insidious onset, pain disproportionate to mechanism, systemic symptoms, and a poor response to previous musculoskeletal treatment — are often the first indication that we are not dealing with a simple mechanical problem.
-
Once layers one through four have cleared, we arrive at the musculoskeletal assessment itself. This is the domain most people associate with osteopathy — and it is where the majority of clinical time is spent. But it is worth noting: everything above is what makes the musculoskeletal assessment safe.
Layer 5 includes:
Postural and movement screening — observation of stance, gait, and active range of motion
Regional orthopaedic testing — joint stress tests, provocation tests, and neurodynamic tests appropriate to the complaint
Palpatory examination — tissue quality, joint mobility, fascial tension, and somatic dysfunction across the relevant spinal regions and periphery
Functional assessment — how the presentation connects to the patient's activities, loading patterns, and physical demands
This is also where the biopsychosocial context established in the history becomes clinically active — informing how we interpret findings, calibrate treatment intensity, and set realistic goals together with the patient.
The sieve in practice at The Movement Co
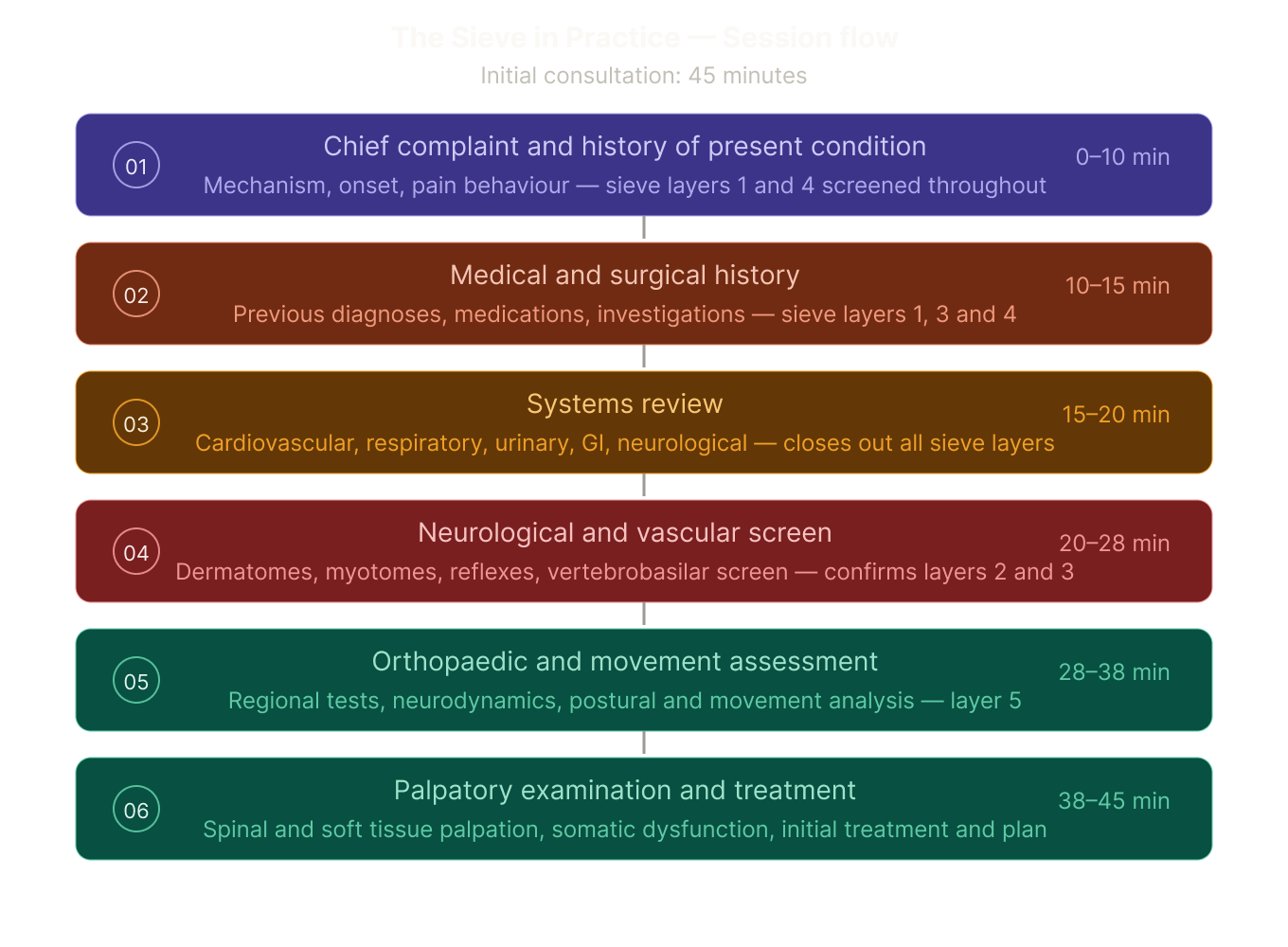
Most patients do clear all the sieve layers in the first 15 minutes or so.
The session flow above shows how the sieve is embedded into the initial 45-minute session — not as a separate interrogation, but woven through history-taking and physical examination in a way that feels like a conversation.
The sieve is not something we do to patients. It is something we do in partnership with them, explaining what we are looking for and why.
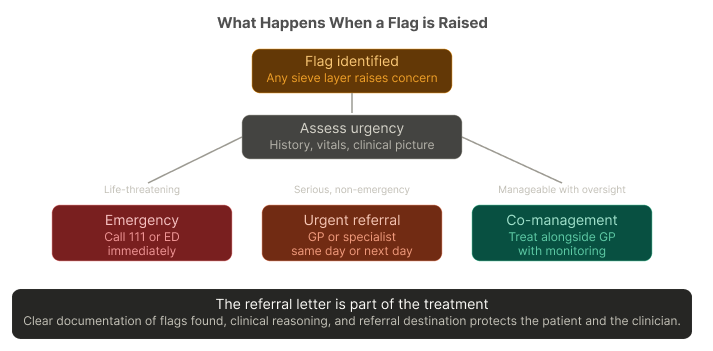
When a flag does emerge, the explanation of why we are referring — and what the referral is intended to achieve — is part of the care.
Most patients pass all five layers in the first 15 minutes.
For them, the sieve is invisible — the history feels thorough, the clinician seems attentive, and the assessment moves efficiently toward treatment.
That experience is the goal.
For the small number of patients where a layer raises concern — where the back pain turns out to be referred renal colic, or the neck pain has UMN signs, or the fatigue and night sweats alongside the shoulder pain warrant an urgent blood panel — the sieve is the thing that changes the outcome. Possibly significantly.
what you can expect at your first appointment
Every initial consultation at The Movement Co follows the osteopathic sieve framework. You will be asked questions that might initially seem unrelated to your chief complaint — your general health, bowel and bladder function, previous medical history, cardiovascular history. These are not irrelevant. They are the most important questions in the room.
By the time we reach the hands-on component of the assessment, both you and the clinician have a clear, evidence-based picture of what is happening, what it is appropriate to treat, and what an honest prognosis looks like.
That is what good osteopathic care looks like.
Not just skilled hands — an intelligent system that uses those hands only when it is safe and appropriate to do so.
"So essentially the first session is as much about ruling things out as finding things to treat."
Freddie: "Exactly. The best clinical decision I can make is sometimes: this isn't mine to treat. And knowing that quickly is the point."
References:
Deyo RA & Diehl AK (1988). Annals of Internal Medicine.
NICE Clinical Guideline NG59 (2016).
Australian Commission on Safety and Quality in Health Care (2018).
IFOMPT cervical artery dysfunction framework (2020).
Greenhalgh S & Selfe J — Red Flags: A Guide to Identifying Serious Pathology of the Spine (2006).