Hypermobility: When Flexibility is not a flex
"Freddie, I have a friend who's incredibly flexible — like, unnaturally flexible. She's always been proud of it. But lately she's in constant pain. How does being flexible cause pain?"
Freddie: "This is one of the most misunderstood things we see. Flexibility without control is just instability. And instability, over time, means your joints are working overtime to hold themselves together. That's exhausting — and eventually, it hurts."
What is hypermobility?
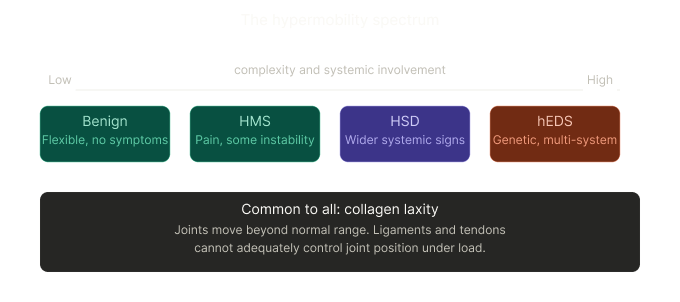
Hypermobility means your joints move beyond their normal range of motion. It happens because the connective tissue — the collagen that makes up ligaments, tendons, joint capsules, and skin — is more elastic than it should be.
For many people, it goes unnoticed for years. You're "double-jointed." You were great at gymnastics as a kid. You can put your leg behind your head. Cool party trick. No big deal.
But for a significant number of people, it comes with a package of problems: recurring sprains, joint pain, fatigue, poor proprioception (your brain's sense of where your body is in space), and sometimes symptoms well beyond the musculoskeletal system — digestive issues, dizziness, skin fragility, anxiety.
This is where hypermobility syndrome (HMS), or its more complex cousin, hypermobile Ehlers-Danlos Syndrome (hEDS), comes in.
The Beighton Score — a simple screening tool
The first clinical step in assessing hypermobility is the Beighton Score. It's a quick 9-point orthopaedic screen that tests joint laxity across five movements. You can do most of it at home as a rough guide — though clinical context always matters.
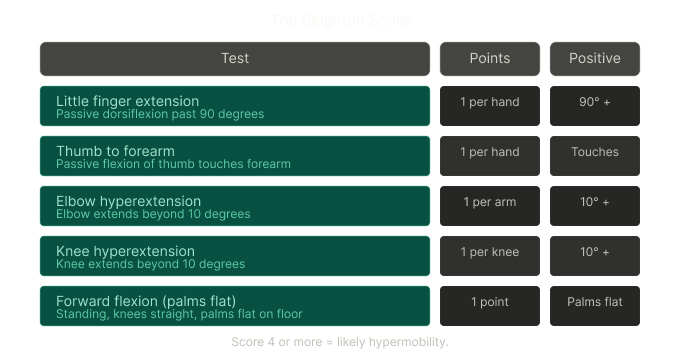
A score of 4 or more out of 9 is considered a positive finding for generalised joint hypermobility. But — and this is important — the Beighton Score is a screening tool, not a diagnosis. It measures how bendy you are. It doesn't tell us whether your hypermobility is symptomatic, how it's affecting your function, or whether a more complex connective tissue disorder is in play.
That's where further assessment comes in.
When to look further — hEDS and the 2017 diagnostic criteria
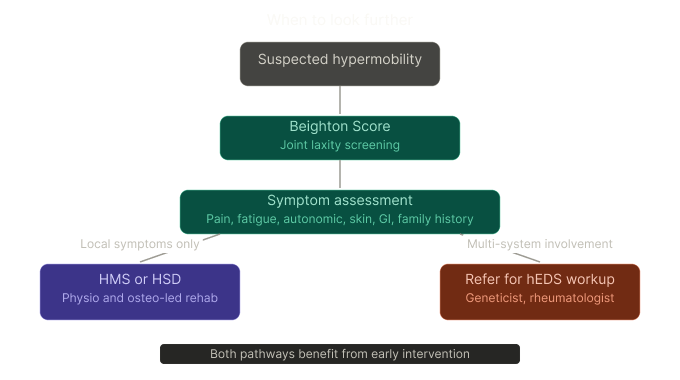
If the Beighton Score flags hypermobility and the person has widespread pain, fatigue, autonomic symptoms (dizziness on standing, gut issues, palpitations), skin changes, or a family history — we need to look beyond the joints.
The 2017 International EDS Classification introduced specific diagnostic criteria for hEDS. Unlike other EDS subtypes, there is currently no genetic test for hEDS — diagnosis is entirely clinical, meaning it relies on a thorough assessment of symptoms, history, and physical findings across three separate criteria sets.
"So what difference does it make catching this early versus finding out at 35 after a decade of unexplained pain?"
Freddie: "It's genuinely life-changing. And I don't say that lightly."
Why early detection matters — a lot
Here's why early detection matters:
If caught early:
Strength and stability programs can be introduced before significant joint damage accumulates
People learn to move in ways that protect their joints — reducing sprains, subluxations, and dislocations
Nervous system sensitisation is less entrenched — pain is easier to manage
Mental health impact is reduced — people know what's happening to their body, which itself reduces anxiety and catastrophising
Children can be monitored through growth phases — which is when symptoms often worsen
Appropriate sport and activity modifications can be made before damage is done
If missed for years:
Chronic widespread pain often develops, sometimes meeting criteria for fibromyalgia
Multiple joint injuries accumulate, some requiring surgery
Fatigue and deconditioning compound — creating a vicious cycle
Anxiety and depression rates are significantly higher in undiagnosed hypermobility populations
People spend years being told their pain is "in their head" or that nothing is structurally wrong — when the real issue is a connective tissue disorder that doesn't show on a standard MRI
The difference isn't just clinical. It's the difference between a person who manages their condition confidently and one who's been failed by the system for a decade.
What The Movement Co does for hypermobile patients
This is a patient group we have a particular interest in, and one that requires a fundamentally different approach to standard musculoskeletal care.
Here's the key shift: with most patients, we're trying to restore mobility. With hypermobile patients, we're trying to build stability. The joints already move too much. The goal is not to stretch — it's to strengthen the muscles that act as the primary stabilisers when the passive structures (ligaments and joint capsules) can't do their job properly.
Our approach:
Full Beighton screening and orthopaedic assessment at intake, with specific loading tests to assess functional joint control — not just range of motion
Identifying which joints are symptomatic and why — not all hypermobile joints cause equal problems
Graded neuromuscular retraining — teaching the nervous system to recruit stabilising muscles earlier and more effectively under load
Blood Flow Restriction (BFR) training — allows meaningful muscle loading at low external weights, critical for hypermobile patients who often cannot tolerate high loads due to joint instability
Proprioceptive training — rebuilding the brain's sense of joint position, which is frequently impaired in hypermobility
Load management — helping you understand your "energy envelope" and avoid the boom-bust cycle that drives so many hypermobile patients into flares
Education and self-management — so you're not dependent on us to stay functional
Referral pathways when warranted — if we suspect hEDS or significant autonomic involvement, we refer appropriately rather than managing in isolation
A note on sensitivity: many hypermobile patients — particularly those with hEDS — have a sensitised nervous system and a history of being dismissed. We take that seriously. The assessment is thorough, the explanation is honest, and the plan is built around your presentation — not a generic protocol.
If you suspect you or someone you know might be hypermobile, a structured assessment is always worth doing. The earlier, the better.
"So you're essentially giving the body the stability it was born without."
Freddie: "Exactly. The joints have more range than the muscles and nervous system know what to do with. We close that gap."