WHAT THE CRACK?
"Freddie, I went to a chiropractor once and he cracked my neck and it felt amazing.
He told me my vertebrae were out of place and he put them back. Was that real?"Freddie: "The relief was real. The explanation was not. And that distinction matters more than most people think."
What is that crack, actually?
Let's start with the sound. The pop or crack that happens during a spinal manipulation is one of the most satisfying sounds in healthcare. And for decades, the assumption was that it meant something had been "put back" into place. A joint. A bone. A vertebra.
That assumption has been comprehensively dismantled by modern imaging research.
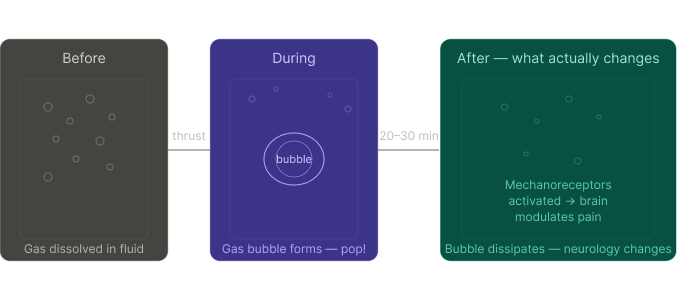
The crack is cavitation — the rapid formation and collapse of a gas bubble inside the synovial fluid of a joint. When the joint is moved quickly through its range under a high-velocity thrust, the intra-articular pressure drops suddenly. Dissolved gases — primarily carbon dioxide — come out of solution, forming a small bubble. The pop is that bubble forming. On fMRI and real-time MRI studies, the bubble can be seen clearly, forming and then slowly dissipating over 20–30 minutes.
The landmark study by Kawchuk et al. (PLOS ONE, 2015) used MRI to capture this in real time in a finger joint — the first clear visual evidence that the crack is cavitation, not structural realignment. The image shows an unmistakable bright void appearing at the moment of the pop.
Nothing moves back into place. The joint surfaces don't shift. The vertebrae don't realign.
What changes is the pressure environment inside the joint — and what happens downstream neurologically from that change is where the real science begins.
Reference: Kawchuk et al., PLOS ONE 2015 — real-time MRI of cavitation
The neuroscience: why manipulation actually helps
If it doesn't realign anything, why does it work?
The answer is neurological. A high-velocity low-amplitude (HVLA) thrust — the formal name for spinal manipulation — triggers a cascade of neurophysiological events that genuinely change how your nervous system processes pain. The relief is real. The mechanism is just completely different from the structural story you were told.
Here is what the research shows is actually happening:
Mechanoreceptor stimulation. The joint capsule and surrounding tissues are packed with mechanoreceptors — sensory nerve endings that respond to movement and pressure. When the joint is moved rapidly, these fire en masse, flooding the spinal cord and brain with proprioceptive input. This effectively "drowns out" nociceptive (pain) signals by competing for the same neural pathways. This is the gate control theory of pain (Melzack and Wall, 1965) in action at the clinical level.
Descending pain inhibition. Studies using fMRI and neurochemical markers show that manipulation activates descending inhibitory pathways from the periaqueductal grey (PAG) in the midbrain — the same system activated by opioids and exercise. Endogenous opioids, serotonin, and noradrenaline are released centrally, producing genuine analgesia that can last hours to days (Bialosky et al., Journal of Orthopaedic and Sports Physical Therapy, 2009).
Sympathetic nervous system response. Manipulation produces a measurable, immediate reduction in sympathetic tone — the nervous system's threat and stress response. Skin conductance, muscle tone, and heart rate variability all shift in ways consistent with a calming of the autonomic nervous system. This is partly why manipulation feels so good: it is genuinely settling the nervous system, not just the joint.
Neuroplastic changes over a course of treatment. Repeated manipulation has been shown to produce changes in cortical representation — essentially rewiring how the brain maps the affected body region. This is relevant for chronic pain, where the cortical map has often become distorted or sensitised.
None of this requires anything to "go back into place." The joint position before and after manipulation is identical on imaging. What changes is the neural environment.
The placebo is real medicine — and the theatrics matter
There is one more layer to the story that the honest clinician has to acknowledge: the crack sounds impressive, and that matters clinically.
The loud pop, the immediate sensation of release, the drama of a high-velocity thrust — these are not irrelevant to outcomes.
They are part of the therapeutic encounter, and phenomenologically, they work.
The placebo response is not "all in your head" in the dismissive sense. It is a measurable neurobiological event. Placebo analgesia activates the same descending opioid pathways as the manipulation itself — the periaqueductal grey, the rostral ventromedial medulla, the same endogenous opioid system. Open-label placebo studies (Carvalho et al., PAIN, 2016) have shown that patients experience meaningful pain relief even when explicitly told they are receiving a placebo. The ritual of treatment — the clinical setting, the confident hands, the satisfying sound, the practitioner's certainty — all contribute measurably to the therapeutic effect.
The cavitation pop is, in part, a piece of theatre. And the theatre is not nothing. It is a conditioned cue that tells the nervous system: something significant just happened, it is safe to relax now. The Pavlovian dimension of clinical treatment is real and well-documented (Colloca & Miller, Neuroscience and Biobehavioural Reviews, 2011). Patients who have had previous positive responses to manipulation develop a conditioned expectation of relief — and that expectation itself releases endogenous analgesics before the thrust has even been delivered.
This does not make manipulation a trick. It makes it a genuinely multidimensional intervention: partly mechanical, partly neurochemical, partly contextual. What it is not — and what the evidence does not support — is structural. The vertebra did not move. The joint did not realign. But the brain received a clear signal that something changed, and it responded accordingly. Dismissing that as "just placebo" misunderstands both the word and the mechanism. The placebo response is one of the most powerful analgesic systems the body has — and a skilled clinician who understands it is not deceiving their patient. They are engaging every available tool.
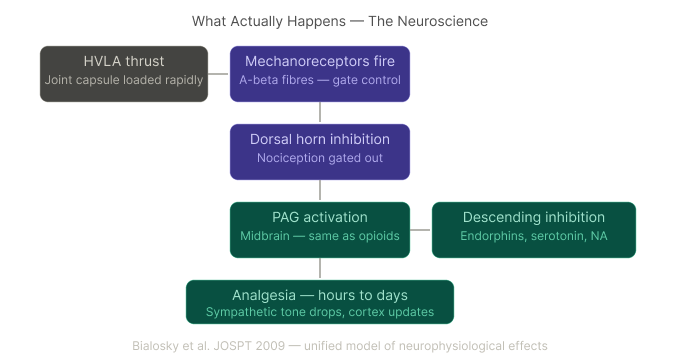
Bialosky et al. JOSPT 2009 — unified model of neurophysiological effects
Fryette's laws and the 33-segment load distribution
Now for the structural side of the story — and this is where osteopathy brings something genuinely elegant.
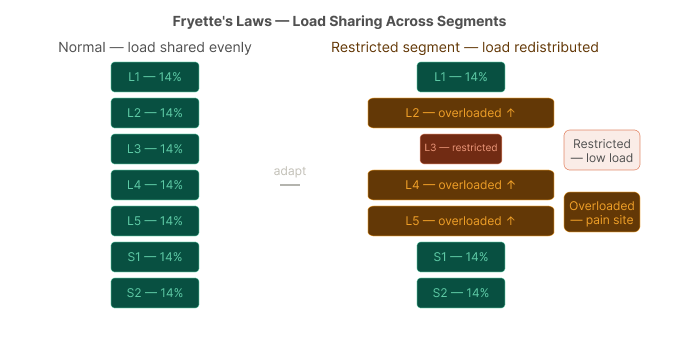
Fryette's laws of spinal mechanics, developed by Harrison Fryette in the early 20th century and expanded in the osteopathic tradition, describe how the 33 vertebral segments of the spine distribute load and movement cooperatively. The spine is not a stack of independent blocks. It is a coupled, interdependent system where movement in one segment affects — and is compensated for by — movement in adjacent and distant segments.
The key clinical implication: when one segment becomes hypomobile (stiff and restricted), adjacent segments must move more to compensate. The load that the restricted segment should be sharing gets transferred to its neighbours. Over time, those neighbouring segments become hypermobile — moving more than they should, their stabilising structures working overtime, their mechanoreceptors increasingly sensitive.
The painful segment is often not the restricted one. It is the one that has been overworking as a compensation.
This is a completely different model from "it slipped out and we put it back." It says: the spine spreads its load across 33 segments by design.
When one segment fails to contribute its share, the whole system adapts — and the adaptation, sustained long enough, becomes the problem.
Fryette HP (1918). Principles of osteopathic technique.
The painful segment ≠ the restricted segment.
This is the clinical art of osteopathy — finding not where it hurts, but why it hurts, and which segment is failing to contribute.
Restoring mobility to a restricted segment, within this model, is not "putting things back."
It is redistributing load — giving the overworked neighbours a rest, and asking the stiff one to start contributing again.
The manipulation isn't repositioning anything. It is changing the neural environment of a restricted joint — releasing the protective muscle guarding, flooding the segment with proprioceptive input, and allowing the body's own load-distribution system to recalibrate.
Should we manipulate? The clinical decision
Not every joint should be manipulated.
Not every patient is a candidate.
The decision requires careful clinical reasoning — and when the answer is no, we have other tools.
The decision flowchart below is the framework we use at The Movement Co.
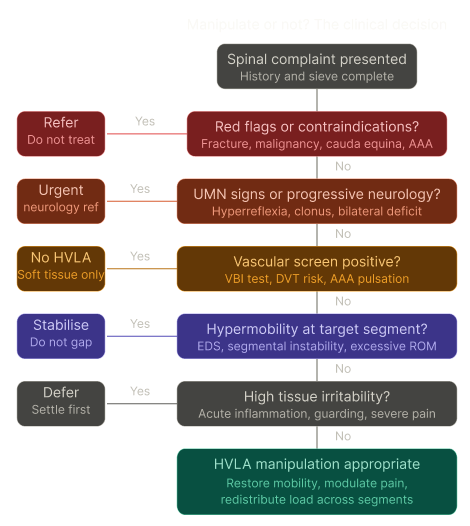
HVLA = high-velocity low-amplitude thrust. Based on IFOMPT guidelines and osteopathic clinical reasoning framework.
the art and the science
The crack is not the treatment. The crack is a side effect of a mechanical event that triggers a neurological chain reaction.
The relief is real — but it comes from your nervous system, not from anything being relocated.
What osteopathy at its best is doing, particularly through Fryette's lens, is asking a more sophisticated question than "what is out of place?"
It is asking: which segments are not contributing their share?
Where is the system compensating?
And what is the least invasive way to restore normal load distribution across the whole spine?
Sometimes that is a high-velocity manipulation. Sometimes it is sustained soft tissue work, mobilisation, or muscle energy technique.
Sometimes — when the joint is already hypermobile, when the tissues are acutely irritable, when vascular risk is present — it is deliberately choosing not to thrust, and working elsewhere instead.
The science and the art of osteopathy converge on the same point: the spine is an integrated system of 33 segments, and we are intervening in a system, not unscrewing a bolt and tightening it back up.
"So when my neck cracks, nothing is actually going back in?"
Freddie: "Nothing was ever out. But something real just happened — and now your nervous system feels it."
References:
Kawchuk GN et al. (2015). PLOS ONE.
Bialosky JE et al. (2009). JOSPT.
Melzack R & Wall PD (1965). Science.
Carvalho C et al. (2016). PAIN.
Colloca L & Miller FG (2011). Neuroscience and Biobehavioural Reviews.
Benedetti F (2008). Nature Reviews Neuroscience — neurobiology of placebo effects.
Fryette HP (1918). Principles of osteopathic technique.
IFOMPT cervical artery dysfunction framework (2020).
Pickar JG (2002). J Electromyogr Kinesiol — neurophysiological effects of manipulation.