Can You Breathe?
At-Home Tests for Respiratory Health
"Freddie, I can breathe fine. I'm not gasping. Why would I need to test my breathing?"
Freddie: "Because most people who breathe badly don't know they breathe badly. It just looks like anxiety. Or neck tension. Or not sleeping well. Or fatigue during exercise. Breathing is the most under-assessed system in the entire body."
Breathing and pain — a connection most clinics miss
There is a strong and well-established relationship between dysfunctional breathing and musculoskeletal pain. A 2014 systematic review by Dimitriadis et al. in the Manual Therapy journal found altered respiratory mechanics in patients with chronic neck pain. The diaphragm serves a dual role — breathing AND spinal stabilisation. When breathing is inefficient, the diaphragm cannot fulfil both roles simultaneously, and the neck, shoulders, and lower back compensate. This perpetuates pain.
Hyperventilation — over-breathing — drops CO2 in the blood, causing vasoconstriction, reduced oxygen delivery to muscle tissue, and nervous system sensitisation. In effect: poor breathing turns up the pain dial.
These tests give you a meaningful window into how well your respiratory system is actually functioning.
-
How to do it: Sit quietly for 5 minutes. Without counting consciously, have someone else count your breath cycles (one inhale + one exhale = one breath) for 60 seconds while you read or look at your phone. Self-counting tends to alter breathing rate.
What it means:
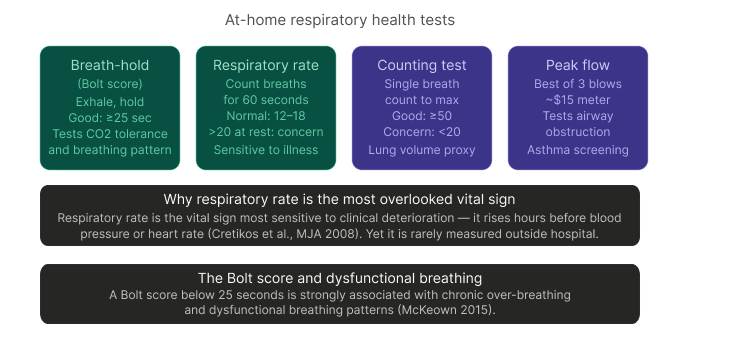
12–18 breaths/minute: normal adult range
Below 12: slow; seen in very fit individuals or those with certain neurological conditions
Above 20: clinically elevated; associated with acute illness, anxiety, respiratory disease, or chronic hyperventilation
Cretikos et al. (Medical Journal of Australia, 2008) established that respiratory rate is the vital sign most sensitive to early clinical deterioration — rising hours before other parameters change. Yet in routine health monitoring, it is almost universally ignored.
-
The Bolt score was developed by breathing researcher Patrick McKeown, drawing on decades of Buteyko breathing research, as a practical measure of CO2 tolerance and breathing pattern efficiency.
How to do it: Sit relaxed. Take a normal breath in through your nose. Let a normal breath out through your nose. Then pinch your nose closed and start a timer. Stop the timer at the first definite urge to breathe — not the maximum hold you can endure. Breathe normally again.
This is a sensitive first-line indicator of over-breathing. Use the interactive scale above to interpret your score. A score below 25 seconds is consistent with dysfunctional breathing patterns and is common in people with chronic pain, anxiety, fatigue, sleep disturbance, and post-viral conditions.
-
Developed as a simple clinical bedside tool, the counting test gives a rough index of vital lung capacity without any equipment.
How to do it: Take the deepest possible breath in. On a single exhalation, count aloud at a steady pace — "one, two, three..." — until you completely run out of air. Count your maximum number.
What it means:
50 or above: normal lung volume for most adults
30–49: mildly reduced; worth monitoring
Below 20: significant reduction; seen in obstructive conditions (asthma, COPD) or restrictive conditions (post-COVID, scoliosis, neuromuscular disease); warrants GP investigation
Reference: Hinds and Watson, Intensive Care, 1996. Also used in respiratory physiotherapy as a simple bedside screen.
-
A peak flow meter costs approximately NZD $15–20 at most pharmacies and gives you a direct measurement of how fast air exits your lungs — the primary test for airway obstruction in asthma and COPD monitoring.
How to do it: Stand upright. Take the deepest possible breath in. Seal your lips around the mouthpiece and blast out as hard and fast as you can. Record the number. Repeat three times and take the best score.
Compare to your predicted peak flow, calculated from height, age, and sex — calculators are freely available online (e.g. UK Nuffield Health PEF calculator). In general:
80–100% of predicted: normal
60–80%: mild-moderate restriction; worth GP discussion
Below 60%: significant obstruction; seek assessment
In people with asthma, a morning dip in peak flow (testing on waking) greater than 15% compared to evening readings is a validated clinical indicator of poorly controlled airway disease.
Reference: Nunn AJ, Gregg I, BMJ 1989 (normative PEF data).
The breathing-pain connection at The Movement Co
Breathing retraining sits within our scope of care — particularly for patients with chronic neck and shoulder pain, anxiety-linked pain, post-surgical deconditioning, and persistent fatigue. When we identify dysfunctional breathing patterns during assessment, we address them directly.
The diaphragm is a postural muscle. It stabilises your lumbar spine before your arms or legs move.
If breathing is compromised, movement is compromised — and so is your pain.
A Bolt score below 20, a resting respiratory rate above 18, or poor counting test performance are all findings worth bringing to your next appointment.
"So breathing — something I do 20,000 times a day — might actually be what's winding up my pain?"
Freddie: "For a significant number of people? Absolutely yes."
References:
Cretikos MA et al., Med J Aust 2008;
Dimitriadis Z et al., Manual Therapy 2014;
McKeown P, The Oxygen Advantage 2015;
Nunn AJ & Gregg I, BMJ 1989; Hinds CJ & Watson D, Intensive Care 1996;
Kolar P et al., J Orthop Sports Phys Ther 2010 (diaphragm as postural stabiliser).